

Author: Professor Barry Doyle (University of Huddersfield)
In the years before the creation of the National Health Service (NHS) the hospitals of England were divided between two providers – acute and specialist voluntary institutions treating a range of mostly curable conditions and a much larger number of municipally controlled establishments providing isolation for infectious diseases or with roots in the nineteenth century poor law. On the eve of the Great War these providers drew their patients from distinct socio-economic groupings with patients segregated between paupers and the respectable sick poor, men and women, adults and children, the acute and the chronic, the dangerous and the safe, the old and the young, the curable and the incurable.

Architect’s Impression of the Completed King Edward VII Extension, Leeds, 1917
(Edward VII Memorial Appeal leaflet, West Yorkshire Archives, Leeds 2295/299)
Further distinctions emerged with the finance and management of institutions and from the way the medical staff were appointed. Voluntary hospitals drew their income from subscriptions, gifts, donations and legacies from local elites supplemented by some democratic community and workplace fundraising. Their management reflected this – small boards dominated by the subscriber elite – while their patients often secured admission through an element of patronage. The medical staff, in keeping with this charitable profile, gave their services for free acquiring status and private patients from their honorary positions.
Public hospitals were left to deal with the social groups and conditions excluded by the gatekeeping practices of the voluntary establishments. Local authorities were obliged to protect their communities from the infectious and the mentally ill. The sick wards and infirmaries of the workhouse took care of the rest. The fact that these services were paid for by local taxation limited their development as did the belief that the conditions and people dealt with were socially, physically or morally suspect or dangerous. Moreover, management roles carried less status and power while the salaried nature of the small number of medical staff meant they were viewed with suspicion. As a result the two systems rarely cooperated, both sides resisting efforts to integrate in the interests of either efficiency or the patients.

New Operating Theatre, St James’ Hospital, 1940
(Brochure for the Opening of the Extensions at St James’ Hospital, Leeds, West Yorkshire Archives 2295/390)
Yet over the following thirty years the segregation by class, age, gender and condition associated with the pre-war system began to break down in the face of a democratization of the funding base, changing political conditions, increasing pressure on beds and the transfer of power from traditional elites to the medical staff. A major financial crisis immediately after the First World War led many voluntary hospitals to either set charges or attempt to secure a contribution from patients. In some parts of the country, especially heavy industrial areas (but also London) pre-payment mutual schemes were established ensuring free treatment for members when admitted. This move coincided with the collapse of the subscriber recommendation system of admission and its replacement by medical criteria with access to a bed mainly decided on medical need rather than elite patronage.
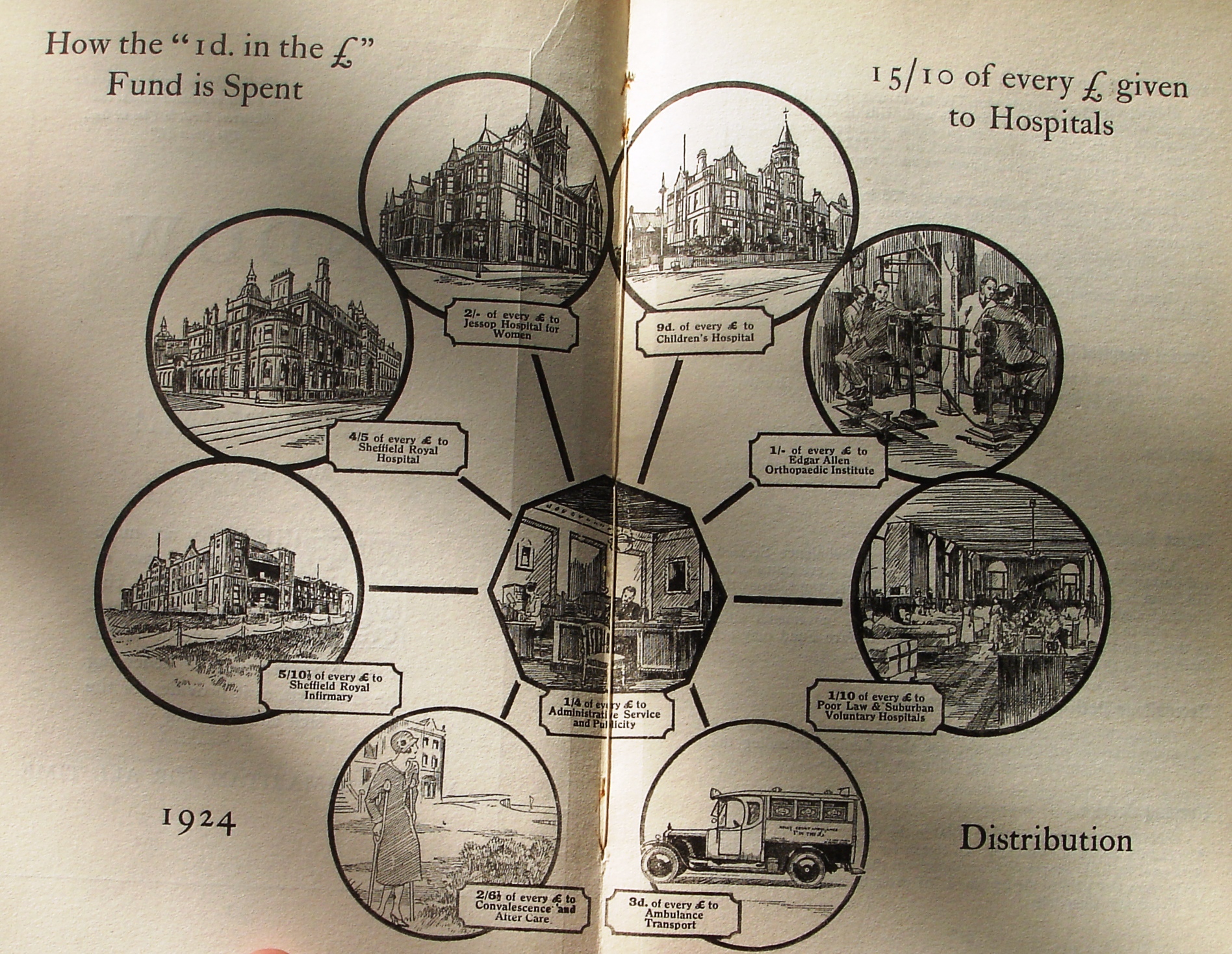
‘How the Penny in the £ Fund is Spent’
(Sheffield Hospitals’ Council, Third Annual Report, 1924)
The democratization of funding and the ascendancy of medical criteria for admission put huge pressure on the resources of the voluntary hospitals leading to over-crowded wards and ever lengthening waiting lists especially for minor or mundane conditions. Yet at the same time most workhouse medical provision was under-utilized. At the end of the 1920s, the government abolished boards of guardians and transferred their responsibilities to councils. As a result some local authorities developed their poor law infirmaries as general hospitals admitting non-pauper patients at a small charge. Many urban poor law infirmaries were re-branded as municipal general hospitals and began to expand their services to include extensive maternity provision, the appointment of consultants, the undertaking of minor surgical procedures and the development of some specialties. This move has sometimes been seen as a competitive challenge to the voluntary hospitals if not an outright act of aggression. Yet in most cases this was not the case and indeed the emergence of the municipal general hospital permitted the incorporation of an increasing number of patients into an integrated local hospital system which distributed cases by medical need rather than perceived financial or social status.
Although historians have questioned the extent to which collaboration followed the abolition of the poor law, in the case of Leeds and Sheffield there is evidence of joint working driven by local contributory schemes, patient demand, political will and medical professionals. In both cities, around 5,000 patients were being treated in municipal hospitals at the expense of the mutual schemes by the end of the 1930s. Despite initial concerns that members would not want to be admitted to the supposedly inferior municipal general, the sick showed little discrimination, preferring treatment – often by the same doctors – to waiting for a voluntary hospital bed. This seems to have been the case particularly amongst women, seeking treatment for minor ailments or wanting to have their babies in hospital.
But integration was also being promoted by the doctors. In Leeds consultants were being appointed to the poor law infirmary before it was taken over by the council while from the mid-1920s the medical superintendent was increasing the number of operations undertaken. More significantly, the superintendent was working closely with the admissions ward of the Leeds General Infirmary to sort and allocate patients and from 1936 this became policy across the city. Similar arrangements were made for maternity cases after 1936 – with the voluntary hospital taking first time mothers and complicated cases while the municipal hospitals admitted ‘ordinary’ births. In Sheffield arrangements in 1930 saw a specific number of cases transferred to the municipal hospitals at the expense of the council while it was agreed that additional maternity beds and a casualty unit would be built by the local authority and the city divided into three zones for the allocation of accidents and emergencies. Integration was most widely canvassed in the case of those conditions requiring acute surgical or specialist therapies and long term care, especially cancer treatment by radium which was moving towards collaboration by 1945.
An artist’s impression of the Graves Radium Institute, Sheffield, c.1945
T.W. Barnard, Memoir on the Origin and Progress of the Trust, (pp Sheffield 1964)
Thus, even before the NHS came into being in 1948 it is apparent that, in urban areas at least, much of the segregation which had characterised the pre-Great War hospital system had given way to a more integrated approach. Relatively few patients found their way into particular institutions because of who they were and the majority were admitted first and foremost on medical grounds, usually meeting their obligation to contribute directly or indirectly to their care.
For more on changing hospital provision in Leeds and Sheffield see Barry Doyle, The Politics of Hospital Provision in Early Twentieth Century Britain, is available from Pickering and Chatto.

Reblogged this on CHPHMblog and commented:
This post by Barry Doyle, Director of the Centre for the History of Public Health and Medicine, forms part of a series of short examinations of segregation and integration in hospital provision posted in preparation for the forthcoming conference of the International Network of the History of Hospitals in Dubrovnik in April 2015. Look out for the announcement of the programme very soon.
An interesting discussion is definitely worth comment. There’s no doubt that that you need to write more on this subject, it might not be a taboo matter but generally people don’t discuss these subjects. To the next! Kind regards!!